At the iwCLL (International Workshop on CLL) held this past October in Edinburgh, Scotland, I caught up with Dr. Neil Kay to discuss some of the recent research on predictive and prognostic markers in chronic lymphocytic leukemia presented at the biennial conference.
Takeaways:
- The value of FISH, IgVH mutation status, and TP53 testing is already well established and should be part of the care of all CLL patients.
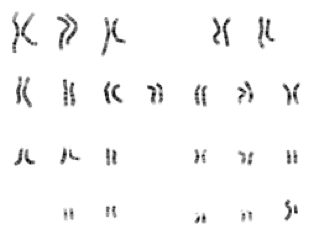
- Karyotype refers to the number and appearance under a microscope of the chromosomes in the CLL cells’ nuclei. See the picture below of a normal male karyotype.
- This is an old-school test that involves a scientist peering down a microscope at cells that have been caught in the middle (metaphase) of their division or mitosis. This is when they are easiest to see and count.
- It requires cells to be dividing and since CLL cells are slow to divide, it has not been an easy or standard test to do until recently when we have found new ways to stimulate the cells to divide.
- There is no standard way to measure karyotype in CLL, so this test is still experimental.
- Complex karyotype (CK) traditionally refers to when there are 3 or more aberrations in the 23 chromosomes. These abnormalities may include:
- deletions, including del 17p, where the short arm of the 17th chromosome is missing.
- an extra chromosome, as in trisomy 12, where there are 3 instead of the normal 2 copies of the 12th
- a translocation, when apiece of one chromosome breaks off and attaches to another chromosome. This is rarer in CLL than is some other cancers.
- There is controversy about whether 3 or 5 in the right number of abnormalities to best use for prognostication in CLL.
- For more research on this, please see this CLL Society article where the study coordinators, Drs. Panagiotis Baliakas and Kostas Stamatopoulos, stated:
- “By definition, complex karyotype is present when there are at least three structural or numeral aberrations on the chromosomes in a given sample. However, a noteworthy finding from our study was that patients with five or more aberrations had a shorter overall survival than those with three or four, independently of other factors.”
- CK does suggest a worse prognosis, but the extent that it is an independent risk factor and not linked to FISH and other findings, is a matter for future research.
- For more research on this, please see this CLL Society article where the study coordinators, Drs. Panagiotis Baliakas and Kostas Stamatopoulos, stated:
Conclusions:
There is something, at least to me, that seems comforting and grounded about a lab scientist using a light microscope to tell us about how well or badly our chronic lymphocytic leukemia is likely to behave. If it looks weird, it acts weird.
I like to think of CK as a marker of how likely our CLL cells are to mutate. If, by the time we take a look, they have already made the microscopically visible karyotype “complex” with 3 or more changes, odds are the cells will continue to mutate, increasing the odds that they “mutate” around the blockades thrown up by medications, and the disease will be harder to treat.
This also explains why there is a link between CK and deletion 17p and TP53, the gene that control the fidelity of the gene replication process. When they are missing or mutated, copying of genetic material can go awry and there are no consequences to the increasingly aberrant cells.
At this time, karyotyping is still mostly a research tool, but that might change soon.
Please keep in mind that these genetic changes we are discussing are only happening in the CLL cancer cells and not in the rest of the body. 23andMe genetic tests won’t be seeing complex karyotypes.
Here is a video of my interview with Dr. Kay from iwCLL 2019:
This is a “working” meeting with no accessible press rooms for interviews, so please pardon our background noise.
Thanks for your attention.
Stay strong
We are all in this together
Brian
Dr. Brian Koffman, a well-known retired doctor, educator, and clinical professor turned patient has dedicated himself to teaching and helping the CLL community since his diagnosis in 2005. He serves as the Executive Vice President and Chief Medical Officer of the CLL Society Inc.
Originally published in The CLL Society Tribune Q4 2019.
















