Dr. Rick Furman of Weill Cornell, in NYC has a long and deep experience treating CLL with novel therapies.
At ASH 2018, I interviewed Dr. Furman on how to best use the novel agents to treat CLL.
We will focus on the many non-chemo options available these days that include:
- Single agents (one drug at a time), usually ibrutinib
- Fixed duration of a combination of approved novel therapies
- Clinical trials of single or combinations of yet to be approved meds or combinations not yet approved
There still is a small role for chemo-immunotherapy (CIT) on its own and some exciting research where we can reduce the amount of CIT given and greatly improve efficacy by adding an oral targeted drug such as ibrutinib or duvelisib to FCR, but we will review that elsewhere.
Based on the latest research and his experience and expertise, here are some of Dr. Furman’s key opinions on how to treat CLL.
Takeaways:
- Use the best treatment you have when it is needed. In other words, don’t save therapies for later.
- This is especially true when it comes to the strategy by some community hematologists to use CIT frontline and “save ibrutinib” as a rescue therapy. This is a bad idea for many reasons including the fact that the most important factor for predicting a durable response to ibrutinib is absence of del 17p. Del 17p only occurs in 4-7% of frontline patients, but is found in 35-40% of patients who have relapsed after CIT. So, if one uses CIT frontline, one significantly increases the risk that ibrutinib will be less effective. Ibrutinib is a better drug when used frontline.
- Nearly all patients who can tolerate single agent ibrutinib frontline and who don’t have del 17p have not progressed after more than 7 years and 80% of all the patients have not progressed.
- To get that to 100%, combinations should be considered, but the added benefits need to be balanced against the possible increased risk of side effects. Remember that some combinations are not helpful such as adding rituximab to ibrutinib.
- There are many combinations in trials right now and we don’t know yet what the best mix will prove to be.
Conclusions:
Few doctors have more experience that Dr. Furman in treating CLL with novel agents, so I listen carefully to what he has to say.
Treatment approaches are changing fast, so today’s best practice may be sorely out of date in the near future.
That is why it is critical to have a CLL expert on your team who is aware of the latest research and able to offer appropriate trials.
There is no perfect pathway to treat CLL and every case is different, but the treatment choice should be informed by the latest research and the patient’s preference.
Here is my interview with Dr. Furman where can you find many details about the recent results and ongoing trials:
Dr. Furman referenced several papers from ASH. Here are a few of the many links to the abstracts themselves or interviews with the researchers.
Here is the impressive data for those treated with ibrutinib alone.
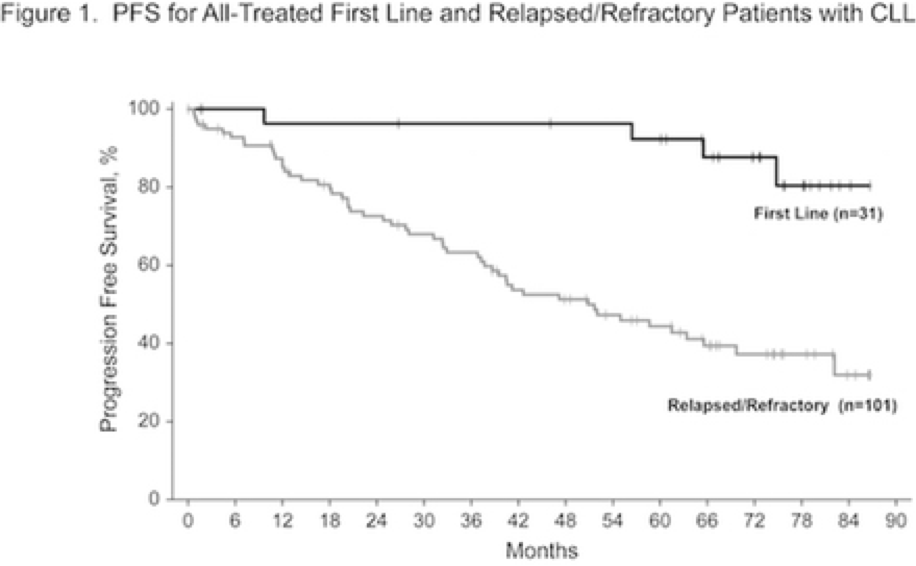
Here is link to that abstract: http://www.bloodjournal.org/content/132/Suppl_1/3133
Here is Dr. Jain on Dr. Nitin Jain on a fixed duration of Ibrutinib and Venetoclax in Treatment-Naïve High-
Here is the ASH 2018 update on this same trial.
There are so many good choices.
Thanks
Brian
Brian Koffman MDCM (retired) MS Ed
Co-Founder, Executive VP and Chief Medical Officer
CLL Society, Inc.
















