We are in a very much welcomed downward trend in COVID-19 case numbers, hospitalizations, and deaths right now. However, it is important to understand that the virus is still out there and future surges and new variants are sure to come.
Many hospital systems and healthcare entities are suddenly removing their mask requirements for staff right now. This is concerning for those with CLL / SLL who are immunocompromised and seeking healthcare. Some other options might be to again consider telehealth visits as appropriate. If you must be seen in person, CLL Society would highly encourage you to advocate for yourself by calling ahead of any healthcare (or dental) visits to make a special request for any healthcare providers who are going to be in direct contact with you during your exam to remain masked. They should still be able to make these reasonable accommodations for you, even if masking is no longer required by their state health department or healthcare system.
COVID-19 Statistics
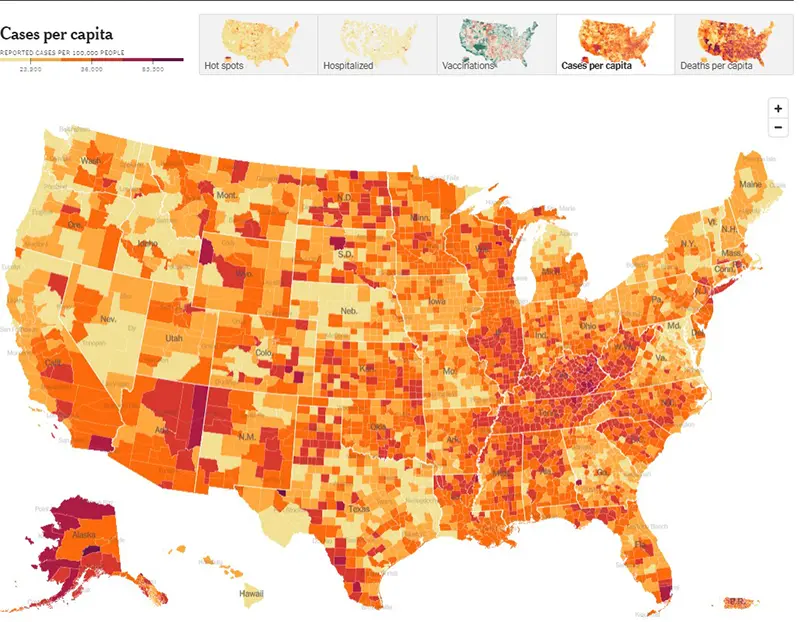
Here is this week’s CDC map of community level of spread (this particular link is weighted based on hospitalizations and not based upon the actual level of community spread). And here is the link to the New York Times actual cases per capita map as pictured below. The New York Times data was last updated March 5th. As you can see there are still several hot spots around the country.
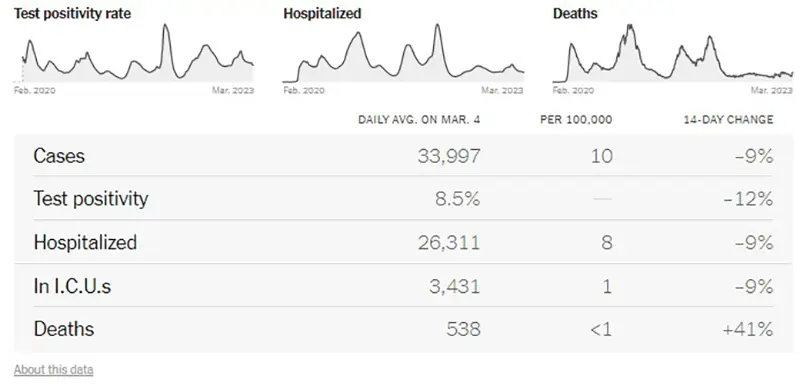
Here is the summary graphic from the New York Times as of March 5th. We continue to see a downward trend in all 14-day change metrics, except for deaths have taken a sudden sharp increase over the past two weeks.
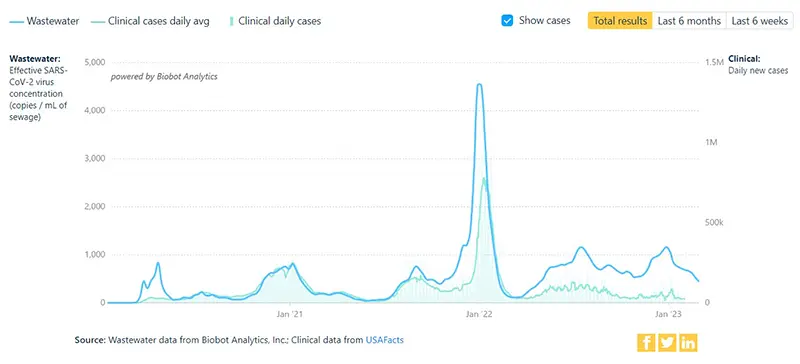
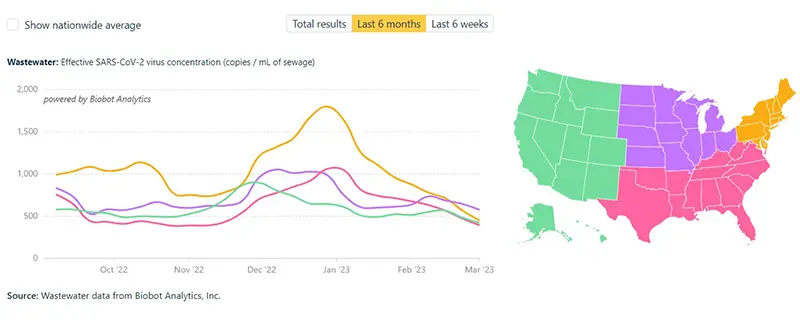
Here is a graphic from the Wastewater Monitoring Project last updated on March 2nd. This graphic reflects a slight decrease in the amount of SARS-CoV-2 virus being detected in wastewater, but also indicates we may be hitting a plateau at the highest level we’ve seen since the beginning of the pandemic.
The additional graphic below from the Wastewater Project shows SARS-CoV-2 viral concentrations by region. All regions reflect a downward trend with the highest concentration of SARS-CoV-2 virus concentration amounts now being found in the Midwest region of the country.
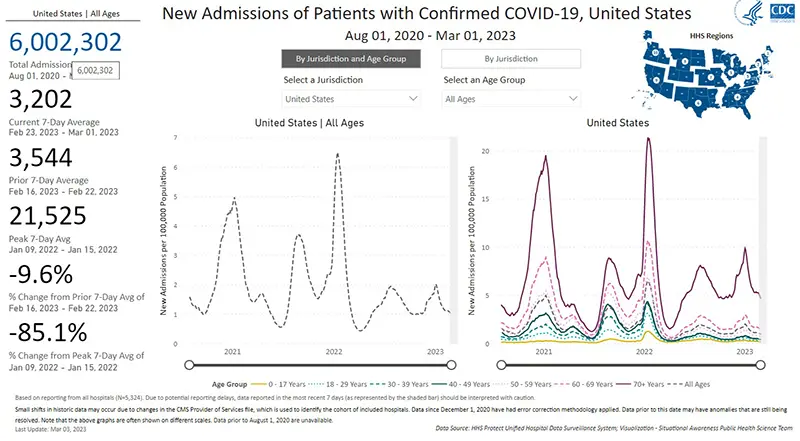
Hospitalizations due to COVID-19, last updated March 3rd, overall appear to be plateauing as well (gray dotted line graphic on the left) and are down 9.6% from the week prior. Although hospitalizations by age group have all gone down compared to the peak of the winter wave, there continues to be a disproportionately high number of hospitalizations for those over the age of 70 (purple solid line on the right) compared to all of those in younger age groups.
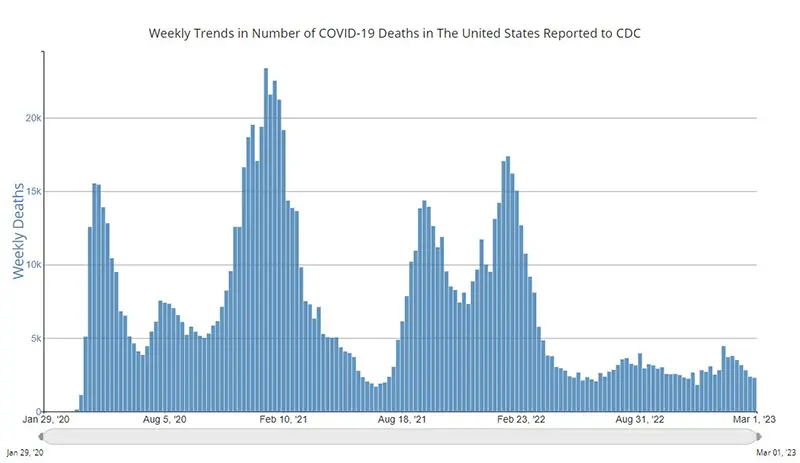
The weekly average number of COVID-19 deaths according to the CDC in the US ending March 1st were 2,290. This is a slight decrease from 2,368 the week prior. Note that this data reported from the CDC is a couple of days behind the New York Times data that was mentioned above (notating a more recent increase in COVID-19 deaths). But the CDC data tends to provide more of a real-time trend by showing what has happened in the previous week (versus the NYT’s being based on a 14-day trend).
Current & Emerging Variants of Concern (VOC)
As of March 4th, the XBB.1.5 variant (also called the Kraken variant) makes up 90% of total new cases in the US according to the CDC Variant Tracker. There are still no other variants that are showing significant gains (which is good news for now).
XBB.1.5 has swept across the country and makes up nearly all of the variant proportions nationally.
COVID-19 in the News
- An article came out in Nature about a COVID-19 pill called ensitrelvir (not yet approved in the United States), which shortens symptoms in people with mild COVID-19 and is thought to reduce the risk of long-COVID.
- It was announced in a press release that a new COVID-19 monoclonal antibody produced by Invivyd that is intended to prevent (and possibly treat) COVID-19 in immunocompromised individuals, will enter into a Phase 1 clinical trial during the first quarter of 2023. Once aligned with regulatory authorities, additional clinical studies are planned to follow.
- An article in JAMA again highlights that surviving the acute phase of COVID-19 is not the only hurdle for many, and that there is an increased risk of adverse cardiovascular outcomes which can occur up to one year following infection. The risk for all-cause mortality doubled (this included heart attacks, strokes, pulmonary embolism, deep vein thrombosis, and other adverse cardiovascular outcomes) in the year following COVID-19 infection when compared with matched uninfected control groups. These adverse outcomes occurred regardless of whether the individual was hospitalized for their COVID-19 infection, meaning the two-fold increase occurred even in those who had mild infection. These data replicate many previous studies and are yet another reason that avoiding COVID-19 infection (and reinfection) altogether remains extremely important.
- The CDC published in their Morbidity and Mortality Weekly Report (MMWR) a study that analyzed wastewater taken from international flights during the fall of 2022. Wastewater samples for the flights tested indicated 81% of were positive for SARS-CoV-2 virus. This only supports what we already knew in that masking requirements on planes should not have been discontinued, flying remains a high-risk activity, if you must get on an airplane an N95 mask should be worn at all times.
Immunocompromised and worried about COVID-19? If you recently had your COVID-19 vaccine booster, you may be eligible for free antibody testing to understand your antibody levels, as part of a research registry for potential participation in a COVID-19 prevention study of investigational monoclonal antibody therapies. Click here to learn more.
Keep learning, and please stay well.
Robyn Brumble, MSN, RN
Director of Scientific Affairs & Research
CLL Society