 By Laurie Adami – Patient
By Laurie Adami – Patient
I am Laurie Adami and I grew up in the Northeast, moving to the Boston area when I was in high school. I attended Colgate University majoring in Russian language and international relations. After graduating, I was recruited by the intelligence agencies but elected to go into financial services instead and accepted a job in the trust department at a large bank in Boston.
In 1984, I packed my car and moved to Los Angeles from Boston to accept a job with a start-up financial software firm. I remained with the same firm for nearly 25 years and assumed the responsibility of president when the founder retired in 1999.
My life was cruising along, I was married in 1998 and had a son, August (Gus), in 2000 at the age of 40. My career included extensive travel and bi-coastal living in the late 1980s/early 1990s when I would spend 2 weeks each month in Los Angeles and 2 weeks each month in Manhattan. During my career, I amassed 3 million frequent flier miles on American Airlines.
When my son was just 4, I began to experience health problems – extreme fatigue, frequent sinus infections and bronchitis, and a swollen node in my neck. I also developed very dry eyes and was no longer able to wear my contact lenses.
Unfortunately, the doctors I saw during this time were not responsive to my concerns. They asked me about my lifestyle and work and told me they would be exhausted too if they were doing what I was doing. My blood work was all normal and I was told if my bloodwork was normal, it was unlikely anything was seriously wrong with me. I saw a series of doctors and was tested and found negative for an autoimmune disorder, Sjogren’s syndrome. I was told I must have developed seasonal allergies even though all the allergy testing I underwent was negative.
Still seeking answers, my son was now in kindergarten. I had felt something in my abdomen and had been told by a doctor that it felt like a hernia and I shouldn’t worry about it. At the end of my wits, I fired all of my doctors and was referred by a friend to an internist who specialized in diagnosing patients. He agreed that what I felt in my abdomen was likely a hernia but said “we don’t guess about these things; this is why we have CT machines”. I was sent the next day for a CT scan – I was told it wouldn’t require any contrast but before I had even put my clothes on to depart the imaging center, they brought me bottles of contrast to drink. My heart plunged.
Two days later, on Good Friday, 2006, at the age of 46, I learned I had stage IV follicular non-Hodgkin lymphoma, an incurable blood cancer. The lump I felt in my abdomen was not a hernia but was a mass larger than a grapefruit. The enlarged node in my neck was lymphoma and I had lymphoma in my lungs and throughout my body. My tear ducts were blocked with lymphoma – explaining my painful dry eye.
A third opinion doctor I saw regarding treatment options suggested that I had a 50% chance of being alive in two years. He couldn’t understand why I broke down in tears when he told me that statistic. My son was only in kindergarten and he might not have a mom before he was in third grade. I was enraged and left his office, never to return.
I immediately started brute force chemotherapy, R-CHOP, and after I completed the 6 cycles, obtained a complete remission. Sadly, at my first follow-up scan just 3 months later, I had already relapsed.
Between 2006 and 2017, I had 6 different therapies, including two chemotherapies, experimental radioimmunotherapy, an HDAC inhibitor, monoclonal antibodies, and a PI3 kinase inhibitor. Two of these treatments were clinical trials and I was in continuous treatment. Unfortunately, the drugs all ultimately stopped working and I had six relapses.
But I carried on, ever hopeful that eventually, a therapy would come along that would vanquish my disease.
In 2012, I attended a Leukemia & Lymphoma Society (LLS) event where they described a new immunotherapy called CAR-T (chimeric antigen receptor T-cell) therapy. I was struck by the elegance of the approach. All of my treatments to date were one size fits all man-made drugs. CAR-T utilized a customized approach – my own T cells would be harvested, genetically modified, and reinfused into my body with a target that would see and destroy only cancer cells. I was blown away and told my oncologist that he just needed to keep me alive until CAR-T was available in a trial for follicular NHL.
In March 2018, I was out on a walk when my UCLA oncologist, Sven de Vos, called me to inform me that a Kite Yescarta CAR-T trial, Zuma-5, was opening at UCLA with 5 spots. I would be the first patient in the trial and immediately went to UCLA to sign the trial paperwork.
By this point, my cancer was approaching 10 pounds and my face was unrecognizable. I also had a kidney blockage and was running out of time. I knew I was at great risk of significant side effects from the CAR-T cells as it appeared there was a correlation between disease burden and side effects. The more disease, the more side effects. At that point, the methods to control side effects were not well developed. But I had no other options, so I had nothing to lose really.
My T-cells were harvested in mid-June 2018 and sent to the lab at Kite Pharmaceutical for genetic modification. One month later after an unsuccessful attempt to shrink the size of my disease and the three days of lympho-depleting chemo to make room for my T cells to be infused and expanded, I entered the Ronald Reagan Hospital at UCLA. On July 16, 2018, the 24th anniversary of the day I met my husband, Ben, I received my CAR-T cells back. The reinfusion was less than 15 minutes long. My oncologist estimated that they had removed one million of my T cells and they were modified and expanded to about a billion cells.
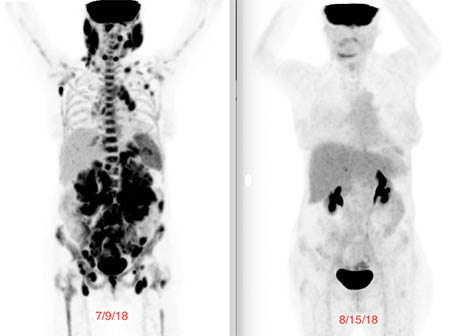
Two days later, grade IV cytokine release syndrome (CRS) set in – very high heart rate, low blood pressure, a fever of 105 degrees. I was moved to the ICU for 3 days where I was pumped full of fluids and stabilized. Back on the transplant floor, I began to experience CAR-T related encephalitis syndrome and experienced a dozen brain seizures. At that point, I was placed in a medically induced coma. I was in the hospital for 36 days, which included 25 days in the ICU and over a week in a coma. On August 15, 2018, still ensconced in the hospital, I was wheeled down to the PET CT scanner. Miraculously, in just 30 days, every single one of my tumors had disappeared. I am attaching images here that show the dramatic transformation. On the left is the scan just one week prior to my getting my CAR-T cells back. The scan on the right is one month after.
In July, I had my 2-year post CAR-T PET scan and remain in complete remission. My 12 years of “scanxiety” is finally fading away as it appears, I have a durable remission. All of the side effects I experienced during my CAR-T hospitalization have vanished and I feel better at 60 than I did at 40!
Since my diagnosis, I have been very involved with LLS. Selfishly, I knew if I raised money for them it could fuel further research that might save my life. LLS has invested over $40 million to date in CAR-T research. They were the first to fund CAR-T research at UCLA and the University of Pennsylvania, where the first two FDA-approved therapies were developed.
Recognizing, CAR-T doesn’t work for everyone and there is still much work to be done to expand its use in additional blood cancers, solid tumors, and even autoimmune disease, I am training to trek to the Mount Everest Base Camp with two of my UCLA oncologists, Sven de Vos and John Timmerman, to raise money for more immunotherapy research. My fundraising goal is $250,000 and you can find information about my journey, join my team and make a donation at www.bit.ly/CarTSupergirl
We were supposed to go in April 2020, but Coronavirus shut down Nepal and the World. We hope to go in the fall of 2021, assuming there is a CV vaccine.
Some people move on after cancer, but having dealt with it for 12 years, it’s hard to move on. I have chosen to try to help others, to raise hope and awareness. I am an LLS First Connection volunteer and speak to numerous patients, providing words of support, guidance, and most importantly, hope.
I am forever grateful for all of the medical staff that helped me over the years, the research facilities that invent these therapies, and the pharmaceutical companies that get these therapies to the patients.
My son, who was in kindergarten when I was first diagnosed, left for his freshman year of college in Washington D.C. by himself the day after I was released from UCLA post CAR-T. He has his emergency medical technician certification and is an EMT at his university.
Laurie retired from her financial services career at her first relapse to focus on her health. She was on the Wells Bring Hope Board of Directors for 8 years -the mission is drilling water wells in rural Niger, West Africa. She also joined the Board of Directors of Audit Integrity/GMI Rating and was on the board for several years until the sale of the business to MSCI. Laurie is currently actively fundraising for The Leukemia & Lymphoma Society whose funding of CAR-T research was lifesaving to her. She is an LLS First Connection volunteer reaching out to newly diagnosed or relapsed blood cancer patients to give them support. She also is a volunteer advocate with the LLS Public Policy group, advocating for legislative changes to benefit cancer patients in Sacramento and Washington, D.C.
















