 We have a cancer of the lymphatic system so it is important to know what that means.
We have a cancer of the lymphatic system so it is important to know what that means.
We will start with a basic explanation of the major component of the lymphatics, namely what exactly are our lymph nodes (sometimes called lymph glands).
Normal lymph nodes are usually about 1 cm in their longest dimension but can be much smaller, and are oval or bean-shaped.
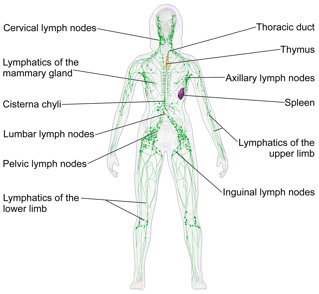
We probably have about 500 to 700 nodes in our body. No one knows for sure. They are part of our immune defense system and so are strategically located in our neck, groin, axillae (armpits), mediastinum (central chest), and pelvic and abdominal cavities to guard the portals where threats, especially pathogens that may try to enter the core of our body.
 They are well supplied with lymph and blood vessels that allows for the easy entrance or departure of the lymphocytes that live there. That explains what happens when some “signal blocking” medications such as ibrutinib and idelalisib cause our cancerous lymphocytes to leave the glands: our lymph nodes dramatically shrink while our blood lymphocyte count rapidly climbs.
They are well supplied with lymph and blood vessels that allows for the easy entrance or departure of the lymphocytes that live there. That explains what happens when some “signal blocking” medications such as ibrutinib and idelalisib cause our cancerous lymphocytes to leave the glands: our lymph nodes dramatically shrink while our blood lymphocyte count rapidly climbs.
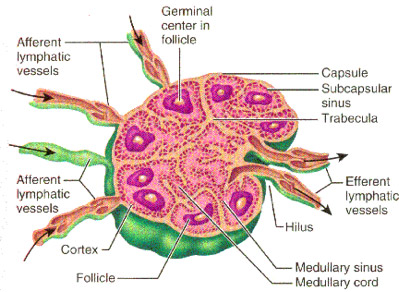
Healthy lymph nodes are structured in a way that provides an ideal environment for communication between the immune cells that are necessary for proper activation of the T and B lymphocytes that are required for defense against certain bacteria, viruses and parasites.
The outer layer or cortex contains the B-cell areas, or follicles. That is where our cancerous CLL cells hang out. The middle layer is mostly made up of T cells and dendritic cells. When there is a potential threat, lymph nodes are the place where there the dendritic cells present danger signals (usually a fragment of protein from a pathogen) to a T cell that recognizes the danger, then multiplies and co-ordinates the body’s immune response. Some of the T cells migrate to the follicles to tell the B cells that a problem is afoot and it is time to mature, proliferate and make antibodies.
No wonder our lymph nodes swell in response to an infection or cancer.
CLL is a cancer of the B cells that tend to both live too long and proliferate when there is no real threat. The success of the new “signal blocking” medications is due to their ability to prevent the cancerous B cells from receiving the messages in the nodes to “live long and prosper”. The CLL cells can no longer pick up the signals and so they leave the supportive and safe neighborhood of the nodes for the relative isolation of the blood stream where they eventually die off.
Dr. Brian Koffman, a well-known doctor, educator and clinical professor turned patient has dedicated himself to teaching and helping the CLL community since his diagnosis in 2005. He serves as the unpaid medical director of the CLL Society Inc.
Originally published in The CLL Tribune Q4 2015.
