Authored by Brian Koffman, MDCM (retired), MSEd
Bottom Line:
CLL patients who received BTKi and stopped therapy for non-CLL progression reasons reported an improved quality of life and prolonged time off treatment. This supports the value of prospective studies of time-limited Bruton’s Tyrosine Kinase Inhibitor or BTKi treatment for Chronic Lymphocytic Leukemia (CLL).
Who Performed the Research and Where Was it Presented:
Dr. Deborah Stephens from U. of North Carolina led a distinguished group of researchers including CLL Society’s own Dr. Brian Koffman and Liza Avruch in publishing Feasibility of Bruton’s Tyrosine Kinase Inhibitor Discontinuation in Chronic Lymphocytic Leukemia: The Patient Perspective in Clinical Lymphoma Myeloma and Leukemia on May 16, 2025.
Background:
BTKi (ibrutinib, acalabrutinib, zanubrutinib, and pirtobrutinib) therapies have revolutionized care in CLL, but patients often stop treatment due to reasons other than that it stops working and the CLL progresses. This most commonly due to intolerance of the side effects of the medication. In another chronic leukemia, chronic myelogenous leukemia (CML), the standard for many years was continuous therapy for as long as the medication, another type of kinase inhibitor, was working, until it was proven that these medications could safely be stopped in most patients. Similar studies have not yet been done in CLL and little is known about what happens to patients who discontinue BTKi for reasons other than progression.
Methods:
Between March and May 2024, CLL Society promoted a survey on its website and through its social media channels to patients who self-reported stopping their BTKi for reasons other than CLL progression.
Results:
- A total of 220 surveys were started, but for various reasons the data from only 170 patients was usable and included in the analysis.
- Of the included patients, 57% received their first BTKi in the frontline setting.
- The first BTKi received included ibrutinib (79%), acalabrutinib (17%), and zanubrutinib (4%).
- BTKi was discontinued in < 6 months, 6 to 12 months, 1 to 2 years, 2 to 4 years, and > 4 years in 19%, 18%, 21%, 28%, and 14% of participants, respectively.
- The most common reasons cited for discontinuing BTKi were toxicity (62%), CLL in remission (14%) and personal choice (8%).
- The most common adverse events (AE) that led to BTKi discontinuation were:
- atrial fibrillation (20%)
- arthralgias or joint pains (17%)
- bleeding/bruising (11%).
- Of those who discontinued BTKi due to AE, two out of three reported that it resolved quickly, in a month or less.
- Almost another quarter of patients reported that the AE at least partially improved after discontinuation.
- When asked their perception about stopping the BTKi, the majority of patients:
- were relieved that they be free of side effect side effects (45%)
- were able to focus less on their CLL (11%)
- would no longer have to pay for the medicine (7%).
- However, 29% experienced anxiety about discontinuation.
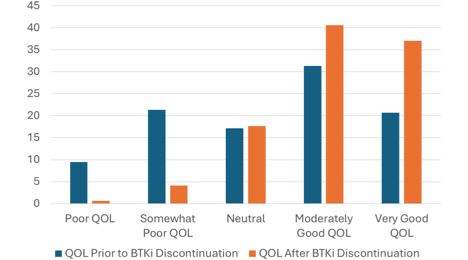
- A statistically significant increase in perceived quality of life (QOL) was observed from prior versus post BTKi discontinuation. On other words, patients’ QOL improved after treatment
- Forty-five percent (76/170) of patients reported no disease progressed. The majority were more than a year out from stopping therapy with 32% out one to two years and 27% out more than two years.
- In the patients who did experience CLL progression by either noting increasing white blood cell counts or enlarging lymph nodes (n = 80), 46% reported that these events did not happen for ≥ 1 year after BTKi discontinuation.
- Those that were on a BTKi for ≥ 2 years before discontinuation had more time without CLL relapse.
- While a new CLL treatment was started in the first six months after stopping a BTKi in 36% of patients, a full half of all the patients did not need to start a new treatment for one year or longer after discontinuation.
Discussion and Conclusions:
Despite the limitations of the data all coming from patients volunteering to complete an online survey promoted by CLL Society, this study does suggest the feasibility for many patients of stopping their BTKi for reasons other than progression, especially for those who have been on the medication for two years or longer. The majority should see an improved QOL and may enjoy a long time of medication before they need treatment again. It also demonstrates the feasibility of the CLL Society community working together to produce peer reviewed clinically relevant research and we are very grateful to all those who participated in the survey.
Resources:
Read the full publication at: Feasibility of Bruton’s Tyrosine Kinase Inhibitor Discontinuation in Chronic Lymphocytic Leukemia: The Patient Perspective.
