Chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL) is an immune compromising illness with infection being one of the greatest causes of morbidity and mortality. Of the several strategies to reduce the risk of infections, vaccinations play a key role in protection against certain transmissible infectious diseases. The goal of this article is to provide guidance to help you make informed choices, although individuals should seek the counsel of their own physicians for specific advice.
Unfortunately, due to defects in immune competence some if not most individuals with CLL / SLL may not produce a strong or long lasting response to a vaccination. However, vaccines still provide varying degrees of protection and thus remain an important facet of medical care and should not be avoided. Furthermore, it is recommended that your household and close contacts be vaccinated as these individuals with intact immune systems are likely to produce a more robust immune response and will add an additional layer of protection around you.
How Recommendations for Vaccinations are Developed
For years the national recommendations for vaccines have been uniformly brought forth by a select group of highly trained specialized medical and public health experts appointed to the Advisory Committee on Immunization Practices (ACIP) under the oversight of the United States Department of Health and Human Services (HHS). These experts through rigorous literature review, analysis and vetting of data and extensive debate annually reviewed and developed vaccination guidelines which were then presented to the Centers for Disease Control and Prevention (CDC) for review and final approval of national guidelines. In turn, the major medical societies which provide primary care services including the American College of Physicians, the American Academy of Family Physicians and the American Academy of Pediatrics subsequently in near uniformity adopted those recommendations. However, since 2025, with many changes afoot internally at the HHS and CDC including the dismissal and replacement of experts on the ACIP, not all of the medical societies now agree with or endorse the most recently updated national recommendations and many organizations have already or are in the process of drafting their own guidelines. However, for adults with immune compromise which includes those of us with CLL / SLL, at the present time the various medical societies appear mostly to be in agreement with the CDC and ACIP recommendations. Many of the guidelines provided here will be synthesized from CDC guidance, recommendations from medical societies including the Infectious Diseases Society of America (IDSA) and American Society of Clinical Oncology (ASCO), and from supporting medical literature.
Vaccine Classes
Vaccines can be divided into the two classes of non-live and live vaccines. Live vaccines for the most part should not be administered to individuals with CLL / SLL because they contain a weakened living form of a virus that in individuals with compromised immune systems potentially may replicate to cause actual infection. One possible exception may be the JYNNEOS monkeypox vaccine, though it is highly advisable that any decision for that specific vaccine be made in conjunction with a treating specialist. Below is a list of live and live-attenuated vaccines:
| Live Vaccines | |
| Vaccine | Typical U.S. use |
| Adenovirus type 4/7 | Primarily military use |
| BCG | Rare/select situations |
| Cholera oral | Travel/special risk vaccine |
| Ebola (Ervebo) | Special occupational/exposure risk |
| Influenza nasal spray (FluMist / LAIV) |
Seasonal flu vaccine for eligible people ages 2-49 |
| MMR (M-M-R II, Priorix) |
Adult catch-up in nonimmune people |
| Smallpox (ACAM2000) |
Special exposure preparedness |
| Smallpox/mpox* (JYNNEOS) |
Indicated for persons at risk. * This monkeypox/smallpox vaccine is considered safe for persons with immunocompromising conditions as it is non-replicating, but specialist input is preferred in CLL/immunocompromised patients. |
| Typhoid oral (Vivotif/Ty21a) |
Travel vaccine |
| Varicella (Varivax) |
Adult nonimmune vaccination |
| Yellow fever (YF-Vax) |
Travel/special risk vaccine |
Non-live Vaccines
Inactivated vaccines can be divided into two groups: routine and specialized, the latter being for specific situations such as certain types of foreign travel to locations with diseases not commonly encountered in the United States. Specialized vaccinations are beyond the scope of this article which will only cover those that are routinely recommended. The destination, duration of the trip and other factors are used to determine which vaccines are indicated and that information can be found through the Centers for Disease Control (CDC) here: https://wwwnc.cdc.gov/travel. As a footnote, it is important to know that some travel related vaccines are live and therefore are contraindicated.
The subsequent information to be presented below will review the routinely recommended vaccines, though for your reference the complete CDC adult vaccination guidelines can be found here: https://www.cdc.gov/vaccines/hcp/imz-schedules/downloads/adult/adult-combined-schedule.pdf. Please focus on table 2 which specifically deals with immunizations for immunocompromised individuals.
For those of you in other countries it may be best to check your own national recommendations which may not be the same as for the United States.
For those of you in Britain: https://www.nhs.uk/conditions/vaccinations/
For those of you in Australia: https://www.health.gov.au/health-topics/immunisation/when-to-get-vaccinated/national-immunisation-program-schedule
Routine Inactivated Vaccines
COVID-19 Vaccine
- Though not nearly as severe as in 2020 when the novel coronavirus, SARS-CoV-2, first appeared, the virus continues to persist throughout the year with peaks in the winter and summer months. Severe illness and hospitalizations are still possible for those with a compromised immune system and vaccination amongst other prevention strategies is of key importance.
- There are four available COVID-19 vaccines summarized below. Three of these are mRNA vaccines: two mRNA vaccines made by Moderna: Spikevax and mNexspike, and one mRNA vaccine made by Pfizer-BioNTech: Comirnaty. There is one protein subunit vaccine, Nuvaxovid made by Novavax. There was a fifth vaccine, a viral vector product, made by Johnson & Johnson which is no longer available.
|
FDA Currently Approved COVID-19 Vaccines |
|||
|
Vaccine |
Vaccine type |
Manufacturer / FDA approval date |
Dose |
|
Spikevax |
mRNA |
ModernaTX, Inc. |
2025-2026 Formula: single 0.5 mL dose for ages >=12; contains 50 mcg mRNA. |
|
mNexspike |
mRNA |
ModernaTX, Inc. |
2025-2026 Formula: single 0.2 mL dose; contains 10 mcg mRNA. |
|
Comirnaty |
mRNA |
Pfizer-BioNTech Manufacturing GmbH |
2025-2026 Formula: single 0.3 mL dose for ages >=12; contains 30 mcg modRNA. |
|
Nuvaxovid |
Protein subunit, adjuvanted |
Novavax, Inc. |
2025-2026 Formula: single 0.5 mL dose; contains 5 mcg recombinant spike protein plus 50 mcg Matrix-M adjuvant. |
- The three mRNA vaccines use messenger RNA to instruct the body to make the COVID-19 spike protein found on the surface of the virus inducing the immune system to then make antibodies and T-cells to attack that surface protein.
- Novavax, on the other hand, uses an older technology to make the viral spike protein utilizing an adjuvant to trigger the immune system into making antibodies and T-cells to attack the virus.
- The FDA labeling for COVID-19 vaccines has changed for adults since the original approval, and currently is limited to adults with a high risk condition or ages ≥ 65 years.
- Neither the CDC, ASCO or the IDSA have made a recommendation for a particular vaccine. However, a 2026 review in the European Journal of Oncology, states that mRNA vaccines are recommended for persons with CLL / SLL.
- Specifically comparing the Moderna and Pfizer-BioNTech mRNA vaccines, a 2023 prospective study found that CLL patients who received the Moderna Spikevax had 12-fold higher neutralizing antibody titers and 1.7-fold higher response than those who received the Pfizer Comirnaty vaccine. An additional retrospective study reported in 2023 which did not specify the specific formulations of vaccines administered found a higher risk of breakthrough infections in Pfizer mRNA vaccine recipients as compared to the Moderna mRNA vaccine recipients.
- Drilling down further into the Moderna vaccines, Spikevax (mRNA-1273) was the first generation mRNA vaccine produced and it is administered with a 50 mcg dose. mNexspike (mRNA-1283), was the second generation vaccine to be produced, and it is administered with a much lower dose of 10 mcg. A phase 3 clinical trial entitled NextCOVE comparing the two vaccines was conducted in adults ages ≥ 50 years though excluded patients with hematologic malignancies and immune compromise. The study showed that the second generation vaccine, mNexspike, elicits a higher antibody response with fewer injection-site pain reactions than the Spikevax and that both vaccines exhibited a similar safety profile.
- The CDC/ACIP and ASCO recommend 2 updated COVID vaccine doses per season/year, generally 6 months apart. However, there may be a slight modification in timing based on the therapy being received and the full details are listed in the below table:
|
CDC/ACIP COVID-19 Vaccine Recommendations for Immunocompromised Adults, 2025-2026 |
|||
|
Adults/adolescents ages ≥ 12 years with moderate or severe immunocompromise, including hematologic malignancy |
|||
|
CDC/ACIP category |
Recommendation |
Interval / timing |
Notes for hematologic malignancy |
|
General recommendation |
2025-2026 COVID-19 vaccination is recommended based on individual-based/shared clinical decision-making. |
Use the modified schedule for people who are moderately or severely immunocompromised. |
People may self-attest; vaccination should not be denied because of lack of documentation. |
|
Completed an initial COVID-19 vaccine series before 2025-2026 vaccine |
Give 2 doses of 2025-2026 COVID-19 vaccine. |
Dose 1: at least 8 weeks after last prior dose for Spikevax, Novavax, or Pfizer; at least 3 months for mNexspike. |
This is the common schedule for previously vaccinated adults. CDC no longer recommends additional doses beyond these 2 in the 2025-2026 immunocompromised schedule. |
|
Unvaccinated adult, ages ≥ 12 years |
Complete an initial series with a 2025-2026 vaccine, then give 1 additional 2025-2026 dose 6 months later. |
Moderna or Pfizer initial series: 3-dose initial series, then dose 4 at 6 months. |
Choice of product determines the initial-series intervals. |
|
Started but did not complete an initial series before 2025-2026 vaccine |
Complete the initial series with 2025-2026 vaccine, then give 1 additional 2025-2026 dose 6 months later. |
Intervals depend on prior product and number of prior doses; use CDC Table 2c. |
Useful for patients with interrupted vaccination histories. |
|
HCT or CAR-T recipient vaccinated before or during therapy |
Revaccinate as though unvaccinated. |
Start at least 3 months / 12 weeks after HCT or CAR-T, then follow the unvaccinated immunocompromised schedule. |
Applies when >=1 dose was received before or during HCT/CAR-T. |
|
Finite B-cell-depleting therapy, e.g., rituximab, with vaccine doses during therapy |
Revaccination may be considered as though unvaccinated. |
Suggested start is about 6 months after completion of B-cell-depleting therapy. |
CDC says the clinical team should determine degree of immune compromise, need, and timing. |
|
Ongoing immunosuppressive or B-cell-depleting therapy |
Do not delay vaccination solely because the patient is receiving immunosuppressive therapy. |
When possible, vaccinate at least 2 weeks before starting/resuming immunosuppression; for ongoing B-cell-depleting therapy, give about 4 weeks before next scheduled treatment. |
Applies to patients receiving continuing B-cell-depleting or other immunosuppressive therapies. |
|
Conditions included by CDC |
CDC examples include active treatment for hematologic malignancy and hematologic malignancies associated with poor vaccine responses regardless of treatment status. |
Examples listed by CDC: CLL, non-Hodgkin lymphoma, multiple myeloma, acute leukemia. |
These conditions fit the CDC moderate/severe immunocompromise category. |
Source: CDC Interim Clinical Considerations, COVID-19 Vaccination Guidance for People Who Are Immunocompromised, Table 2c, updated November 4, 2025. ACIP = Advisory Committee on Immunization Practices; CDC = Centers for Disease Control and Prevention; HCT = hematopoietic cell transplant; CAR-T = chimeric antigen receptor T-cell therapy; CLL = chronic lymphocytic leukemia.
- Due to the immunocompromising nature of CLL / SLL and associated treatments which may cause further immune suppression, it is possible that an adequate response to the vaccine cannot be achieved. In 2024, the FDA authorized under Emergency Use Authorization (EUA), pemivibart (Pemgarda), a monoclonal antibody, for prevention of COVID-19 as pre-exposure prophylaxis. It is a preventive measure to be given prior to becoming infected, and is not effective if given as treatment once COVID-19 symptoms develop. Pemivibart is administered intravenously at 3 month intervals and should be deferred at least 2 weeks after a COVID-19 vaccination. It is not a substitute for immunization, but instead is to be used in addition as a supportive measure. Both the CDC and IDSA recommend this treatment for consideration by individuals with CLL / SLL depending on the degree of immune suppression. Further information can be found here: https://cllsociety.org/2024/03/new-covid-19-pre-exposure-prophylaxis-option-for-cll-patients/
- Further information about the COVID-19 virus can be found at https://cllsociety.org/covid-19/
Haemophilus Influenzae Type b (Hib) Vaccine
- Haemophilus influenzae type b is a bacterium that can cause serious infections, including pneumonia, meningitis and bloodstream infection, not to be confused with influenza, which is a viral infection also known as the flu. Vaccination to prevent this disease is normally given to children within the first year of life.
- The CDC advises the vaccine only for adults with an anatomically or functionally absent spleen or who undergo a hematopoietic stem cell transplant (HSCT). It is not routinely recommended for all adults with CLL / SLL unless another indication exists. For those with an anatomically or functionally absent spleen, one dose is recommended for adults not previously vaccinated, and, if possible, should be given at least 14 days before spleen removal. The CDC also recommends a 3-dose series for individuals who are undergoing HSCT, starting 6-12 months after successful transplant even if previously vaccinated.
Hepatitis A vaccine – this vaccine is indicated when an additional risk factor is present, though optionally may also be given if desired.
- Hepatitis A is a viral infection of the liver and is usually transmitted through contaminated food and water. Hepatitis A is an uncommon infection in the United States and is more commonly found in less developed nations though sporadic outbreaks do occur here. This vaccine is recommended for individuals with any of the following underlying risk factors: chronic liver disease, HIV, men who have sex with men, homelessness, travel to an area with high or intermediate endemic rates, injection or non-injection drug use, close personal contact with an international adoptee, work settings where exposure is more likely.
- The CDC database of travel destinations of high or intermediate endemic Hepatitis A rates can be found here: https://wwwnc.cdc.gov/travel/destinations/list
- The Hepatitis A vaccine is available as a stand-alone vaccine or in a combination form with the Hepatitis B vaccine. Speak to your physician about getting vaccinated if you have one of the above risk factors or will be traveling to a destination which puts you at risk of exposure to Hepatitis A or if you just prefer to cover all bases and have this vaccine.
Hepatitis B Vaccine
- Hepatitis B is a virus that is transmitted through exposure to blood and certain body fluids. It can cause severe acute liver inflammation and, in some cases, persist causing chronic liver disease and eventually death. Vaccinations for hepatitis B are now routinely given starting at birth, but for those who did not get vaccinated it is recommended that the vaccination series be given in adulthood.
- There are several hepatitis B vaccines available, all of which are equally recommended.
- For previously unvaccinated adults, the CDC recommends vaccinations for all adults ages 19-59, adults ≥ 60 years with risk factors and for adults ages ≥ 60 without known risk factors who wish to receive it.
- In addition, there is a combination vaccine, Twinrix, containing both hepatitis A and hepatitis B vaccines, and this may be a very good choice to provide protection against both viruses.
- In some cases when there is immunocompromise including following a hematopoietic stem cell transplant (HSCT), serologic testing following the vaccine to test for an immune response may be indicated.
Influenza Vaccine
- The viral respiratory infection influenza which may infect the nose, throat and lungs has a higher seasonal prevalence during the winter months. Disease manifestations can range from mild cold like symptoms to in severe cases pneumonia and even death. The CDC estimates that in the United States from October 1, 2024 through April 30, 2025, there were 51 million cases of the flu, 710,000 flu-related hospitalizations and 45,000 flu-related deaths.
- Because flu peaks during the winter months it is recommended to get the influenza vaccine annually upon its release which is usually in late August to early September.
- All of the Food and Drug Administration (FDA) approved vaccines cover the same 3 strains of the influenza virus which each year are determined to be the most likely circulating strains.
- The approved influenza vaccines can be divided into 3 categories: standard, enhanced, live attenuated as outlined in the table below.
|
FDA Approved Seasonal Influenza Vaccines |
||||
|
Category |
Vaccine type |
Abbreviation |
Live? |
Vaccine Names / notes |
|
Standard influenza vaccines |
|
|||
|
|
Egg-based inactivated influenza vaccine |
IIV3 |
No |
Afluria, Fluarix, FluLaval, Fluzone. |
|
|
Cell-culture-based inactivated influenza vaccine |
ccIIV3 |
No |
Flucelvax. |
|
Enhanced influenza vaccines |
|
|||
|
|
High-dose inactivated influenza vaccine |
HD-IIV3 |
No |
Fluzone High-Dose; one of the 3 vaccines preferentially recommended by CDC/ACIP for adults >=65. |
|
|
Adjuvanted inactivated influenza vaccine |
aIIV3 |
No |
Fluad; one of the 3 vaccines preferentially recommended by CDC/ACIP for adults >=65. |
|
|
Recombinant influenza vaccine |
RIV3 |
No |
Flublok; one of the 3 vaccines preferentially recommended by CDC/ACIP for adults >=65. |
|
Live attenuated influenza vaccine |
Live attenuated influenza vaccine |
LAIV3 |
Yes |
FluMist; live intranasal vaccine for selected nonpregnant people ages 2-49. Not appropriate for immunocompromised patients. |
- The enhanced vaccines produce a stronger immune response than standard vaccines and are generally recommended for older individuals.
- For patients 65 years and older with immune compromise the CDC as well as the 2024 ASCO Guideline recommend Fluzone High-Dose (HD-IIV3), Fluad (allV3) or Flublok (RIV3) as they produce a greater immune response as compared to the standard dose vaccines.
- For individuals less than 65 years of age with immune compromise, the recommendations are less clear. The CDC advises any of the standard dose vaccine or the recombinant vaccine. The 2024 ASCO Guideline for cancer patients less than 65 years of age with a solid tumor or hematologic malignancy (not including those with hematopoietic stem cell transplant) states that there was inadequate clinical evidence to give a preferential recommendation for a high-dose or adjuvanted vaccine, and concluded by saying that individuals should receive whichever influenza vaccine formulation is locally available. The latest IDSA 2025 recommendation for immunocompromised individuals which did not specifically separate out those with hematologic malignancy did state that the high-dose and adjuvanted influenza vaccines may provide a more robust response compared to the other vaccines, though the IDSA did not go so far as to recommend one particular vaccine.
- The live attenuated influenza vaccine, FluMist is contraindicated for persons with immunocompromise.
- Despite having a weakened immune system and a weaker response to the vaccine, immunization may still be beneficial. A 2025 report in the Journal of Infectious Diseases documented influenza vaccination in immunocompromised adults to reduce influenza-associated hospitalization by 32% thus supporting the largely agreed upon recommendation for annual influenza vaccines in this patient population. (Ref: Lewis NM, Harker EJ, Cleary S, et al. Vaccine Effectiveness Against Influenza A(H1N1), A(H3N2), and B-Associated Hospitalizations, United States, 1 September 2023 to 31 May 2024. Journal of Infectious Diseases. 2025;232(4):e626–e636. DOI: 10.1093/infdis/jiaf185. PMID: 40198276.)
Meningococcal Vaccines
- Meningitis is a serious life-threatening illness causing inflammation of the layers surrounding the brain and spinal cord and infection of the bloodstream. There are many different causes, some non-infectious and others infectious including bacterial, viral, fungal and parasitic agents. Vaccines have been developed to prevent a subset of some particular bacteria that can cause meningitis.
- CLL / SLL alone is not a routine CDC indication for meningitis vaccination unless another risk factor exists, such as asplenia, a condition where the spleen is anatomically absent or nonfunctioning, complement deficiency or complement inhibitor use, certain travel, microbiology exposure, outbreak risk, etc.
- There are two commercially available meningitis vaccines:
-
- Meningococcal conjugate (MenACWY) vaccines
- Serogroup B meningococcal (MenB) vaccines
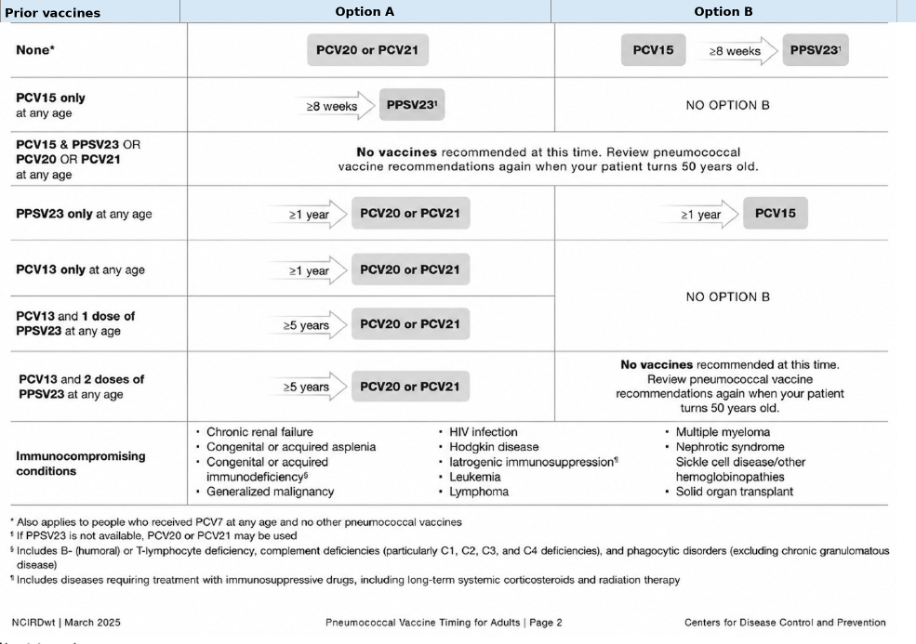
Pneumococcal Vaccines
- The Pneumococcal bacteria, Streptococcus pneumonia, may cause severe life threatening infection with pneumonia, meningitis and blood infection known as sepsis. The vaccine may not prevent infection but certainly may reduce the risk of severe disease, hospitalization and mortality and should be obtained by those of us with CLL / SLL with the best time to get vaccinated being early following your diagnosis of CLL / SLL.
- There are over 90 serotypes of the pneumococcal bacteria and over the years the vaccines have evolved to include different serotypes as indicated by the number following the vaccine name. Older vaccines no longer available include Prevnar 13 (PCV13 ) and Prevnar (PCV7). The four currently available vaccines are Vaxneuvance (PCV15), Prevnar 20 (PCV20), Capvaxive (PCV21) which are conjugate vaccines and Pneumovax 23 (PPSV23) which is a polysaccharide vaccine.
- Because new vaccines have been developed, the guidance has changed over the years and depending on the prior vaccine administered, additional vaccination may be indicated.
- The CDC has divided guidance for pneumococcal vaccination in adults into 3 categories, 2 of which apply to those of us with CLL / SLL. The first is labeled for adults ages 19-49 with immunocompromising conditions. The second is specified for adults ages ≥ 50, annotated with footnotes for immunocompromised persons. These tables can be found here: https://www.cdc.gov/pneumococcal/downloads/vaccine-timing-adults-jobaid.pdf?CDC_AAref_Val=https://www.cdc.gov/vaccines/vpd/pneumo/downloads/pneumo-vaccine-timing.pdf. To simplify what can be confusing vaccine recommendations, I believe it is appropriate for individuals with CLL / SLL who are ≥ 19 years including over the age of 50 years follow the guidance for adults ages 19-49 with immunocompromising conditions and that table from the CDC is listed below.
|
Adults 19–49 years old with specified immunocompromising conditions |
 |
Polio Vaccine
- The scourge of polio has resurfaced in some communities in the United States most likely due to low vaccination rates. The only polio vaccine that has been available in the USA since the year 2000, is the inactivated injected vaccine, or IPV, though many other countries still use a recently updated live attenuated (weakened) oral polio vaccine. Again, CLL / SLL patients should avoid any live vaccines. If you were not vaccinated as a child, which would be most unusual, it would be good to discuss the primary inactivated series with your healthcare team. If you were vaccinated, but travel to, live in or work in a high-risk area, it may be appropriate to discuss with your doctor whether a booster with IPV makes sense.
RSV
Respiratory Syncytial Virus (RSV)
- RSV is an exceedingly common pathogen that causes a respiratory tract infection ranging from the nose to the lungs. Illness can range from symptoms of a mild cold with nasal congestion and drainage to life threatening pneumonia and death. Those at most risk are children, the elderly and high risk individuals with underlying illnesses including immunocompromise, cardiopulmonary disease, renal dysfunction and diabetes amongst others. It has been estimated to cause approximately 159,000 hospitalizations and 10,000 deaths among adults ages ≥ 65 years in the US annually. Like influenza, RSV has a seasonal pattern from October to March with a peak in December with vaccine timing ideally in late summer or early fall before community spread circulation starts to rise. There is no available treatment except for supportive measures and prevention with vaccination is the best option available.
- The three FDA approved RSV vaccines are:
-
- Abrysvo (RSVPreF): FDA approved for adults ages ≥ 60 years, and adults ages 18-59 years at high risk, and pregnant women at 32-36 weeks gestation.
- Arexvy (RSVPreF3): FDA approved for adults ages ≥ 60 years, and adults 18-59 years at increased risk.
- mRESVIA (mRNA-1345): approved for adults ages ≥ 60 years, and younger adults ages 18-59 years at increased risk.
- The CDC recommends a single RSV vaccine for all adults ages ≥ 75 years and adults ages 50-74 years at increased risk for severe RSV, including those with moderate to severe immunocompromise. In contrast, IDSA guidance is broader for immunocompromised patients, recommending RSV vaccination for all adults ≥ 18 years with immunocompromise.
- At present, the RSV immunization is not recommended as an annual vaccine and is only to be given as a single dose.
- In the FDA approval trials efficacy against lower tract infection within the first season of use ranged from 63%-82% in immunocompetent adults. Two subsequent U.S. studies in immunocompromised adults ages ≥ 60 years found the RSV vaccine based upon a pooled vaccine efficacy rate to be 70% effective against RSV-associated hospitalization in immunocompromised adults. ( 2024;404:1547–1559 And JAMA Network Open. 2025;8(5)e258322.
- In terms of adverse events, significant side effects were not increased in the vaccinated vs. non-vaccinated individuals during the FDA trials with the exception of Guillain-Barré syndrome (GBS) being reported for Abrysvo and Arexvy. Following FDA approval, a post-marketing observational study using Medicare claims data suggested an estimated 9 excess cases of GBS per million doses of Abrysvo and 7 excess cases of GBS per million doses of Arexvy. Based on risk-benefit analysis, the benefit in preventing hospitalization and death is believed to far outweigh the risk of vaccination.
Shingles Vaccine
- Varicella-zoster is a viral infection that is spread through respiratory droplets causing a primary infection known as chickenpox, an itchy rash that progresses from red bumps to fluid filled vesicles, often associated with fever and fatigue. Following resolution of infectious symptoms and signs, the virus does not clear from the body, but instead lies dormant hidden in nerve cells. At a later time, often with advancing age and weakened immunity, the virus may reactivate in a form known as herpes zoster affecting one in three persons over the course of their lifetime. The illness most commonly presents as a painful blistering skin rash known as shingles. However, herpes-zoster may reactivate in the eye, nerves of the face, brain or spinal cord resulting in various complications including vision loss, facial paralysis, long term mental decline, paralysis, and death. Furthermore, up to 10-18% of individuals who experience shingles may develop persistent pain in the area where the rash has resolved known as postherpetic neuralgia.
- The first vaccine developed to prevent herpes-zoster infection was Zostavax which has been discontinued globally as of 2024.
- Shingrix, the currently available vaccine, has been shown to reduce reactivation of the virus in the skin, eye, cranial nerves and central nervous system. In the immunocompetent adult, vaccine efficacy for the prevention of shingles is about 97% for adults ages 50-69 and 91% for adults > 70 years of age. For prevention of postherpetic neuralgia, efficacy is about 91% for adults ages ≥ 50 years and 89% for adults ages ≥ 70 years. For patients with CLL / SLL, the immune response to the vaccine is not as robust, and unfortunately, exact efficacy data for prevention of disease is not available. However, a clinical study in CLL / SLL patients has shown an immune response in both the humoral and cellular pathways to the vaccine in both treatment naïve individuals and those on Bruton tyrosine kinase (BTK) inhibitors though in the latter group there was a lesser effect. (Blood Advances. 2022;6(6):1732–1740.)
- The CDC recommends Shingrix for adults ages ≥ 50 years and immunocompromised adults ages ≥ 19 years.
- Vaccination is recommended for all CLL / SLL patients and if possible before the start of treatment, however, vaccination should not be delayed if on a BTK inhibitor. Timing of vaccination might need to be adjusted or delayed if receiving anti-CD20 antibody treatment and should be discussed with your physician.
- Vaccination is a 2 dose series. The initial dose is followed by a second dose 2-6 months later. However, the interval between the first and second dose may be reduced to 1-2 months if necessary before stronger immunosuppressive therapy is administered.
- Revaccinate with Shingrix if you previously received the Zostavax due to the waning protection from that initial vaccine.
- Proceed with the Shingrix vaccine if you are on antiviral prophylaxis such as acyclovir or valacyclovir as these will not reduce the efficacy of the vaccine.
- If you experience herpes-zoster and have not previously been vaccinated with Shingrix, proceed with vaccination once the acute illness has resolved.
Tetanus Vaccine
- Tetanus is a bacterial infection that causes muscle spasms also known as “lockjaw.” The bacteria reside in the soil and may enter the body through an open wound. Diphtheria is also a bacterial infection that usually spreads via respiratory droplets and causes an illness that usually affects the throat resulting in difficulty breathing but may also affect the skin. Pertussis, also known as “whooping cough” is also transmitted by respiratory droplets and results in violent coughing that can be so severe as to result in fractured ribs. Tetanus and diphtheria are rarely reported in the United States though pertussis remains a more common infection. Tetanus, diphtheria and pertussis vaccination begins in childhood and repeat periodic vaccinations through adulthood are necessary.
- Tetanus containing vaccines are available in two commonly administered adult forms:
-
- Tetanus, diphtheria toxoids vaccine (Td) which protects against tetanus and diphtheria.
- Tetanus, diphtheria, and acellular pertussis vaccine (Tdap) which protects against all three bacteria.
- The CDC recommends that once an adult has received a Tdap, either a Td or Tdap should be given every 10 years. However, a Tdap may be the better choice for a booster to gain protection from pertussis which may be severe in an immunocompromised individual. Furthermore, it may prevent an adult from passing pertussis on to an infant younger than twelve months of age at very high risk for pertussis complications.
- A booster Td or Tdap may be indicated if five years have passed from the prior vaccine for wounds that are not clean or minor. Again, either vaccine is acceptable though a Tdap may be the better option.
Administration Timing of Inactivated Vaccines
The optimal timing for an inactivated vaccine depends in part on the specific treatment being administered. The National Comprehensive Cancer Network (NCCN), ASCO and 7th European Conference on Infections in Leukemia (ECIL-7) have come up with guidance summarized below:
- Vaccinations are most effective prior to treatment initiation and ideally should be given at a minimum of 2-4 weeks before starting therapy.
- Vaccinations can be given during therapy with a BTK inhibitor or venetoclax alone or in combination though response may be reduced.
- Adjustment in vaccine timing is necessary when anti-CD20 therapy such as rituximab or obinutuzumab is administered.
- Seasonal vaccines such as influenza and COVID-19 should be given 4 weeks or longer following the most recent dose and be repeated at least 6 months or longer after completion of therapy.
- Nonseasonal inactivated vaccines (such as pneumococcal, Hib, HepB, Tdap, HPV, etc) should ideally be given 2-4 weeks before starting or 6-12 months following treatment with an anti-CD20 therapy such as rituximab or obinutuzumab. However, there is one exception, the Shingrix vaccine, which can be given 1 month or longer after the most recent anti-CD20 dose.
- IVIG does not interfere with inactivated vaccines and does not affect timing of vaccinations.
Vaccinations For Individuals Undergoing CAR-T therapy
CAR-T therapy which is gaining broader use for CLL / SLL therapy needs to be mentioned. The therapy targets both healthy and malignant white blood cells resulting in profound immunosuppression and essentially a transient loss of the antibody producing B-cells. It is recommended that all necessary vaccines be given a minimum of 2-4 weeks before the initial lymphodepleting therapy is administered. Because the therapy causes loss of immune memory from earlier vaccinations including those from childhood, full revaccination with a large swath of vaccines is necessary while the immune system reconstitutes and recovers. The American Society of Clinical Oncology (ASCO), the American Society for Transplantation and Cellular Therapy (ASTCT) and a review by Reynolds et al. have released general recommendations for vaccinations following CAR-T cell therapy, and the National Comprehensive Cancer Network (NCCN) in early 2026 released extrapolated recommendations for vaccinations based on hematopoietic stem cell transplant to CAR-T cell therapy recipients. I have tried to simplify and consolidate the various recommendations into the below chart. However, recommendations may vary based on physician preference, guideline evolution, individual patient needs and, therefore, it is important to seek guidance from your treating physician.
|
CAR T- cell Vaccine Timing Table |
||
|
Vaccine |
CAR T-cell timing |
Doses / schedule |
|
Influenza vaccine (injectable) |
3-6 months |
1 dose annually |
|
Pneumococcal vaccine |
3-6 months |
3-4 doses: 3 doses PCV, then 1 dose PCV or PPSV23 at 12 months |
|
Tetanus, diphtheria, pertussis |
6-12 months |
3 doses: first 2 at least 4 weeks apart, third 6-12 months after second; then Td/Tdap boosters every 10 years |
|
Haemophilus influenzae type b |
6-12 months |
3 doses |
|
Hepatitis A |
6-12 months |
2 doses, single-antigen, or 3-dose combo HepA/HepB |
|
Hepatitis B |
6-12 months |
2 doses, adjuvanted recombinant, or 3 doses, standard; check anti-HBsAb post-vaccination; repeat series if <10 mIU/mL |
|
Inactivated polio vaccine |
6-12 months |
3 doses |
|
Meningococcal ACWY |
6-12 months |
1 dose if low risk, or 2 doses if increased risk; revaccinate every 5 years if risk persists |
|
Meningococcal B |
6-12 months |
2-dose series if low risk, or 3-dose series plus booster if increased risk |
|
Human papillomavirus |
6-12 months |
3 doses; recommended through age 26 years; shared decision-making ages 27-45 years |
|
COVID-19 |
3-6 months |
At least 1 dose; recommendations continually evolve |
|
RSV |
6-12 months |
1 dose for survivors ages 50 years or older |
|
Recombinant zoster vaccine |
6-24 months |
2-dose series for ages 50 years or older; consider ages 19 or older in cellular therapy survivors |
References for the table:
- Kamboj M, Bohlke K, Baptiste DM, et al. Vaccination of adults with cancer: ASCO guideline. Journal of Clinical Oncology. 2024;42(14):1699-1721. doi:10.1200/JCO.24.00032
- Reynolds G, Hall VG, Teh BW. Vaccine schedule recommendations and updates for patients with hematologic malignancy post-hematopoietic cell transplant or CAR T-cell therapy. Transplant Infectious Disease. 2023;25(Suppl 1):e14109. doi:10.1111/tid.14109
- Shahid Z, Jain T, Dioverti V, et al. Best practice considerations by the American Society of Transplantation and Cellular Therapy: infection prevention and management after chimeric antigen receptor T cell therapy for hematological malignancies. Transplantation and Cellular Therapy. 2024;30(10):955-969. doi:10.1016/j.jtct.2024.07.018
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Prevention and Treatment of Cancer-Related Infections. National Comprehensive Cancer Network; accessed June 10, 2026. https://www.nccn.org/professionals/physician_gls/pdf/infections.pdf
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Survivorship. National Comprehensive Cancer Network; accessed June 10, 2026. https://www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf
In summary, vaccinations are one tool in our treatment strategy to reduce the risk of infection and though we may not produce as strong an immune response to these vaccines as compared to individuals with normal immune systems, we should not delay in protecting ourselves as best we can. Because of our unique situations, our treating physicians may choose to modify current vaccine recommendations and it is best to follow your specialist’s advice. It is also important to be aware that guidelines will likely change due to the rapid pace at which medical science is progressing.
We share in this journey together.
Kim Davidson, MD
Kim Davidson received her Doctor of Medicine degree from the Medical College of Virginia. Following training in Obstetrics and Gynecology, Maternal-Fetal Medicine and Family Medicine, she provided medical care and taught for over thirty years. She is also a CLL patient sharing in this journey.
